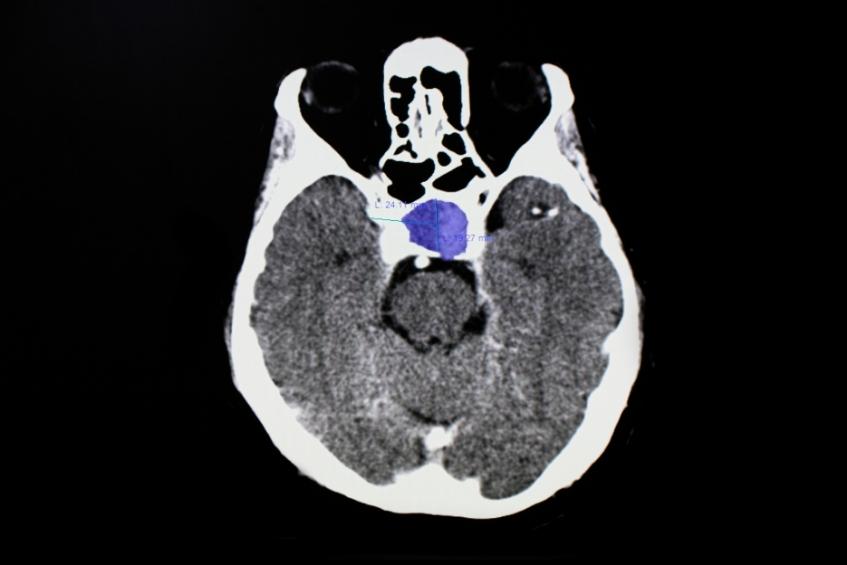
The pituitary gland is a tiny gland that is located inside the skull, above the nasal cavities and beneath the brain. It is located in the sella turcica, a very small bony area. The optic nerves, the nerves that link the eyes and the brain, pass closely above it.
The hypothalamus, an important region of the brain, is directly connected to the pituitary gland. This establishes a crucial link between the brain and the endocrine system, a group of glands that control the hormones in the body. The hormones are released into the blood, which are crucial in controlling the body's organs. The pituitary is considered the “master control gland” because it controls the amount of hormones released by the other glands in the endocrine system.
Pituitary adenomas make up approximately 10% of all tumours that develop within your skull. It affects about 77 out of every 100,000 people, although experts believe that up to 20% of people will develop adenomas at some point in their lives. Due to the fact that many pituitary adenomas, particularly microadenomas, are asymptomatic (producing or showing no symptoms), they frequently go undetected.
Prolactin-secreting pituitary adenomas, known as prolactinomas, are the most common type of functioning pituitary tumour, accounting for approximately 30% of all pituitary tumours. It is a type of tumour that overproduces prolactin, a hormone that stimulates milk production in the breasts. They occur most frequently in females aged 20 to 50 years old, and have a prevalence of 100/million population, and account for less than 2% of all intracranial tumours. It can usually be treated with medication, and surgery would be considered for failed medical therapy.
The causes of pituitary tumours are unknown. Sometimes, gene mutations may increase an individual’s risk for developing pituitary tumours. However, there are no known lifestyle-related or environmental causes of pituitary tumours.
Most people who develop pituitary tumours do not have a family history of the disease. But rarely, pituitary tumours can be a part of hereditary syndromes such as Multiple Endocrine Neoplasia, type 1 (MEN1). Screening for this condition can be done in patients with family history of this disease.
Hormones commonly affected by tumours of the pituitary include adrenocorticotrophic hormone (ACTH), growth hormone (GH), prolactin, thyroid-stimulating hormone (TSH), and luteinizing hormone (LH) and follicle stimulating hormone (FSH). Blood or urine tests can be done to check the levels of these hormones as they may be affected by pituitary tumours. Depending on the type or size of the tumour, there may be deficiency, or overproduction of one or more of these hormones.
Functional pituitary tumours, produce hormones and can cause a variety of signs and symptoms, depending on the hormones they produce. For example, acromegaly can result due excessive growth hormone secretion, or Cushing syndrome may be caused by excessive adrenocorticotrophic hormone secretion.
The signs and symptoms of non-functional pituitary tumours are related to tumour growth and pressure on the surrounding structures. Large pituitary tumours, those about one centimetre or larger, are called macroadenomas. Small tumours are called microadenomas. Because of the size of the macroadenoma, it can put pressure on the normal pituitary gland and adjacent structures, such as the optic nerves and the brain.
Commons signs and symptoms include:
Larger tumours can cause hormonal deficiencies and symptoms which include:
Depending on the type, size and location of the tumour, management options may be surgery, medication, or just regular monitoring by the surgeon. As there are various types of pituitary tumours, there is no single best treatment. Surgery may be done via a transsphenoidal approach, a minimally invasive technique, where the surgeon removes the tumour through the nose, or transcranial, through an opening in the skull, depending on the tumour size and location. In certain cases, Stereotactic Radiosurgery (SRS), a very precise form of therapeutic radiation may be considered.
For smaller tumours, if detected and treated early, the prognosis is extremely good, and most patients will recover and be able to lead a normal life. Therefore, it is important to seek a consultation and get treatment early if indicated.
No, there is no evidence showing that stress may directly cause pituitary tumours, or other tumours in the brain for that matter.
Depending on how badly the optic nerves are affected by the tumour, some fortunate patients may have improved vision after the surgery. However, one of the main aims of the surgery is to prevent the patient’s vision from deteriorating further by removing the tumour compressing on the optic nerves.
Pituitary tumours may grow large and compress on the optics nerves, eventually causing blindness. It may also disrupt the flow of cerebrospinal fluid in the brain, causing it to accumulate in a condition called hydrocephalus. Hydrocephalus is a life-threatening condition and is treated as an emergency requiring surgery. Excessive or deficient hormones in the body may cause physical changes in a person’s appearance, while also affecting blood pressure, blood sugar, menstrual cycle in females, metabolism and sexual dysfunction among other things.
After taking the history of your condition and conducting a physical examination, your doctor will order some blood investigations. This will be followed by an MRI of the brain and pituitary gland. After assessing the results of the investigations, your doctor will explain to you the diagnosis, treatment options, and guide you to decide on the best treatment option for you.

Wait a minute
Wait a minute






